Ventricluar Septal Defects

When Arielle was born on April 25, 2006, 3 weeks earlier than expected, we were so happy to see a healthy baby girl with all of her fingers and toes and lots of pretty dark brown hair. A little short at 17 3/4 ", but at 6 lbs 10 oz. we were pretty happy.

Of course, while Amanda was in labor, they monitored the baby's heartbeat the way they always do, and noticed that it sounded rather irratic. When she was born, they said they heard a heart murmur and kept a close eye on her...
.0.jpg)
...but by the end of the day, they didn't hear anything. We were relieved and thought things were fine.
But the morning they were to leave the hospital, the pediatrician did her discharge check-up and said she was a little jaundiced and heard the murmur loud and clear. They did a chest x-ray and hooked her up to a monitor again. A little scary, but they said she was fine to go home. Again, we were relieved.
But she would have to be hooked up to a "biliblanket" and have a daily blood test until her bilirubin levels came down. It was hard to hold her with that attached to her.
The first couple of days she cried when they pricked her foot for the blood tests. It was such a tiny foot and it was getting so hacked up from all of the tests, the nurse felt guilty having to do it. Of course, the stress level was rising again.
Eventually, she didn't cry; she just got this uncomfortable look on her face, as if she was just accepting this morning ritual as what I'm sure she must have thought was a normal part of life.

Thankfully she recovered from that problem and the daily blood tests stopped. But there was still the heart thing...
On Monday, June 12, she had an appointment with her cardiologist. We were very much relieved that they didn't find it necessary to put her through a cardiocath as her pediatrician had said they might. They did a chest x-ray, electrocardiogram, and an ultrasound. Amanda was told that Arielle has a "medium" sized hole, approximately 3-4 mm, and that her heart is slightly enlarged.
So we are researching this so we'll know what to expect, and here is what we have found so far;
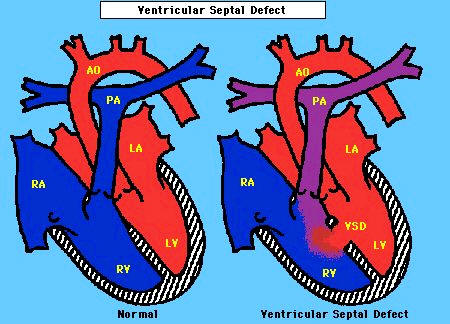
A Ventricular Septal Defect (VSD), or a hole in the heart, is the most common kind of congenital heart defect. It is a hole between the heart's two lower chambers (the ventricles.) The septum is a wall that separates the heart's left and right sides.
When there is a large opening between the ventricles, a large amount of oxygen-rich blood from the heart's left side is forced through the hole (defect) into the right side. Then it's pumped back to the lungs, even though it's already been refreshed with oxygen.
The picture here shows where the hole is commonly located. Arielle's is slightly higher, which I believe the doctor told Amanda is just a little more complicated.
Since the already-oxygenated blood displaces blood that needs oxygen, the heart has to work overtime, pumping more blood, and may cause the heart to enlarge from the added work. High blood pressure may occur in the lungs' blood vessels because more blood is there. Over time, this increased pulmonary hypertension may permanently damage the blood vessel walls.
If the opening between the ventricles is small, it doesn't strain the heart. In that case, the only thing that is abnormal is a loud murmur, and surgery may not be necessary, as they often close on their own eventually.
If the opening is large, even in patients with few symptoms, closing the hole in the first two years of life is recommended to prevent serious problems later. Usually the defect is closed with a patch. Over time the normal heart lining tissue covers the patch, so it becomes a permanent part of the heart. Some defects can be sewn closed without a patch. Repairing a VSD restores the blood circulation to normal and the long-term outlook is good.
Most patients won't need to limit their activity, but if there is pulmonary hypertension or the heart doesn't pump as well as it used to, it might be necessary to limit activity. A cardiologist will help determine if that is necessary.
Most people whose uncomplicated ventricular septal defects are repaired early in life don't have any significant long-term problems. In some people, the heart muscle may be less able to contract. That would require diuretics, agents to help the heart pump better and drugs to control blood pressure.
So... no surgery for now, but she will be seeing the cardiologist often and will most likely have to have surgery when she's 2-3 years old. But it would be so nice if she didn't have to go through that, so we appreciate all of those who are keeping her in your prayers.

The most recent picture I have for now is of Arielle with her uncle; June 26, 2006. But I'll be keeping this updated.
posted by Kim Brownlee at 11:45 PM
0 comments
![]()

